This fall we graduated two cohorts from the Somatic Attachment Psychotherapy 2-year trainings. As we were basking in the glow of the hard and heart work, theirs and ours, we started thinking about getting an insider’s perspective to the training for the BBP blog. We asked for some thoughts, comments, testimonials, whatever people wanted to offer…here’s a few to chew on. Just a quick note to say, we are thrilled with the kind and powerful statements, and blushing just a wee bit.
This is SUCH a brilliantly designed and executed program. I could write a small book about how BBP has strengthened my practice and my life. Each intensive builds on the skills and learning from the one before as the trust and safety in the cohort strengthens. Lisa’s kind and skillful relational guidance allowed me to lean further into the material and into the field in such profound ways. I am so very grateful to have found you and this community!
I strongly recommend this program to any and all counsellors. Attending the BBP 2 yr SAP training course with Lisa Mortimore and Stacy Jensen was simply life changing for me—both professionally and personally. This is hands down the best training I have ever had the privilege to attend and I have taken a lot of training in my almost 20 years in the field! The beautiful blend of solid, foundational academic research combined with witnessing Lisa’s live demonstrations followed by an opportunity to actually practice the skills in each and every intensive made this program invaluable to me. I have grown and healed as a person and am a more skilled counsellor because of my learning and the deeply relational approach that Lisa and Stacy stand by. You will not only gain skills & confidence but you will also become part of an incredible community of committed, skilled, compassionate practitioners. I already can’t wait for the advanced program to begin.
—Tracy Myers, MC, RCC
This training offers the opportunity to become part of a therapeutic community that is rooted in love, where all beings are held with deep respect and dignity. This two-year program offers a gentle layering of skill development and personal transformation, through the ongoing practice of integrating theory, witnessing powerful demonstrations, and practicing skills in a supportive environment. I have come away with so many more resources to use with clients and much more access to my own creativity, lightness, and ease in the work. It is rare to be in the field of such incredible skill and come away with more confidence in ourselves and our own abilities. Lisa brings deep intelligence, humour, humility, and kindness to the practice, encouraging play, experimentation and trust in our clients and ourselves. I’m so grateful for this experience and am looking forward to what comes next.
—Karen Max, MEd, RCC
A few weeks ago a man came to my office after a harrowing work event that left him wondering if he could return. We sat, deeply, tentatively, carefully, and lovingly. Together we found the space and words to heal. He is eager to return to work.
I am deeply grateful to have the foundational aspects of the BBP work to guide my practice, build my knowledge, and ignite the wisdom inherent between the client and me.
Lisa and Stacy and their team offer a well researched, organic, implicit, and authentic approach that supports clinicians to develop the skills to heal clients on multiple levels.
Essential practice.
— Roseanne Cooper MC, AT, RCC
It’s hard to put words to all that I received from the SAP training and cohort. Part way through the training, my nervous system began to respond in new ways to my clients, and to my own internal work. I am continuing to notice somatic responses to material that arises, trusting that my body is processing in new ways with its own wisdom and truth. Integrating this transformation feels invaluable, in addition to strong and clear clinical skills I was able to develop around how to work relationally, with an attachment frame and weaving in somatic skills and practices. The facilitation team was incredibly helpful and supportive, and Lisa’s teaching is precise, deep and offers a unique perspective on the complexity of trauma, soul and spirit and deep ecology. I am deeply grateful for all I’ve received and am excited about the opportunity to deepen in the work with an advanced training. 5 stars!
Happy New Year! I spent my winter holidays mucking about with a few things—catching up on my reading (only fiction over the holidays), clearing out the attic (oh my goodness), making chocolate (with candied oranges and marzipan), taking time with friends, family and feline, and, I had the pleasure of digging into and finishing the A Not So Private Practice podcast (great title!) with hosts Laura Bull and Stephanie Davis, co-owners of Shoreline Counselling (both BBP alumni and facilitators!!!). I was also thrilled to hear a few other shoreline team members (and BBP folks) share their experience of practicing at Shoreline – Amanda Murphy (another BBP alumni and facilitator) and Millie Bata and Mariah Kingston (both currently in the BBP June 2023 cohort).
I laughed, I mean out loud more than a few times…but most of all, I felt good listening to them—talk about stimulating my ventral vagal system😊I was smiling listening to them relate and share their experience of starting, running and growing their group practice. They companioned me as I sorted through boxes of stuff from the attic, and I was entertained, my curiosity was piqued, and I learned a few things about them, about the trials and tribulations of group practice leadership and ownership, about running a clinical practice in terms of marketing, social media, grants/funding etc., and, about how much they love budgeting (who knew). All good stuff.
But, I had two favourite parts, both in the wrap up podcast (but listen to it all, it’s worth it). One, I appreciated their conversation about women and balance, in particular, women who are driven or ambitious, and, I agree, it’s less about balance and more about finding the vitality to live the life you want (and the people to partner with to make that happen – like Laura and Steph have). I also really liked how they framed their relationship—it came up when they talked about their first bad review of the podcast (I couldn’t believe they got a bad review) and that it was someone who didn’t like how much they liked one another, and I loved, I mean really loved, how they framed it, their relationship, as a love story, and it is. Who doesn’t love a good love story? (that’s right from the podcast!!). So, if you are looking for a little lightness packed with wisdom, take some time this winter and listen to season one. I can’t wait until season two!!! Way to go Steph and Laura! http://www.anotsoprivatepractice.ca
I posed a few sentence stems for a free writing exercise this morning at a BBP Somatic Attachment Psychotherapy writing group. What came back was potent, powerful, illuminating, expansive, opening, affirming—you get the drift. We decided to share it…here it goes, enjoy!
I feel confident in my clinical practice…
…when someone says something out loud that has previously been unwitnessed or unspoken.
…when my clients speak their truth, sometimes for the first time.
…when someone says, “I’ve never looked at it that way before.”
…in moments where genuine & healing laughter reverberates through my client’s system as well as my own.
…when clients see my tears in response to their hurt or pain and reflect back the experience of feeling “seen” or “not alone.”
…when clients are able to make changes in their life and relationships as a result of feeling a greater sense of internal steadiness.
…when I am able to provide clients with “a different experience” than they are accustomed to. That is, a different experience related to communication, a different relational experience, or a different experience of connection.Amanda J. Murphy, MC, RCC
This is what I know to be true in my clinical practice: When I meet with someone clinically, I bring in the regulation of my system, my capacity to attune to them and I hold internally the strong belief that through the therapeutic relationship the work in therapy will happen. “Love is Medicine”, a powerful healing balm.Susana Farinha, MC, RCC
This is what I know to be true in my clinical practice: What I know to be true in clinical practice is that being relationally held by another with an open heart heals. I know that the more I journey into my Self, clearing and expanding, the more stability and space I have to be present to the truth and pain of others. If I can be with me and move through what is in the way, then I can be with you more completely. I know the power that exists in the delighted twinkle of an eye, the soft reflection of acceptance, and the comfort of a therapist able to hold all of me. What I know to be true in clinical practice is that embodiment, regulation, and relational connection can actually feel like magic. Rachael Pasemko, RSW, RCC, RPT-S
This I know to be true in my clinical practice: I practice from the heart. I attach. I engage my body as the vessel of connectivity it is intended to be. I hold a space of warmth, welcome, challenge, acceptance, and high regard for innate and intimate wisdom of the soul-ular nervous system. My practice is me & I am my practice. My practice shifts & responds to the changing tides, rhythms, and movements of the Earth, stars, and cosmos, as they signal their need at the subtle energetic level tied vitally to my being. I hold lineage, ancestry, and legacy within my care. I attune to the pulse of the lived & loved ones making the beat of their existence known in the space amongst, within and between us. I play; I hold politic; I navigate complexity. Love is the medicine that awaits all ailments. Time, willingness, and presence to what emerges are the bandages that are Here2Hold & swathe us all.Efré Laurence Divina, MA, RCC
I know this to be true in my clinical practice: I am an advanced therapist who has grown professionally and personally in my years of practice. My commitment to my own development as a person, is an exciting never-ending exploration into the Self. I believe it is not so much ‘what I know or do’ but ‘how I am’ with clients, that can make the difference. I offer my compassionate presence, and a creative space to listen to those on the journey of being and becoming. Dawn Sather, MSW, RSW, RCC
What is true in my clinical practice: I know that as humans, we all have a need for love and connection. We need to feel “gotten” by another, accepted and understood. I know that if I am in a state of loving presence with my clients, in a way that creates a feeling of safety, I can trust that what needs to be revealed in order for my client to heal, will come to the surface to be witnessed and transformed. As children, when our needs are not met: needs for safety, nourishment, connection and attunement, we will create blocks to our own truth and sense of worth in order to manage the incongruence. Although at some level we know that our needs matter, we learn to disavow our own needs and consequently make choices that are not in our best interests. Working relationally in the present moment, with constant attention to nervous system regulation, those blocks to knowing that we are worthy and that our needs matter, can be gradually exposed and removed, and connection to intuitive knowing restored. I know that by holding my client in a space of safety, love and acceptance, eventually, there will be a softening of the protective mechanisms that get in the way of the connection we so deeply desire. From there we can attend to the process of rewiring the patterns that form the internal working model, and be freed to live a more satisfying and loving life.Lana Marie Willow, MA, RCC
This is what I know to be true in my clinical practice: As I write this, I keep coming back to the reality that my clinical practice, and I believe all good clinical practice, is a fluid and living thing, and I can see the many ways that mine has grown and aged and matured, as I have grown and aged and matured. There is certainly bedrock that my practice is built on, (but even tectonic plates move) such as my love for my clients, and my ability to provide quiet love in the Winnicottian sense- to really recognize those who have suffered the Trauma of Non-Recognition. My practice is also dynamic, in the excitement that I feel when I learn a new piece of theory, or read a piece of clinical writing, or make a connection in a session that expands my clinical and heart understanding of why people struggle, and am reminded of the immense potential for relational repair. For me, when these threads of love and learning come together in session, they create a magic moment of possibility for connection and healing that I’m finding impossible to put into words- not wanting to trivialize or lessen the beauty and privilege that I feel for being able to witness it. And this is what I know. Stacy Adam Jensen, MEd, RCC
This is what I know to be true in my clinical practice: I know I can lean into my relational capacity, my ability to find connection and common ground, a meeting place. I can trust my capacity to witness, to hold, to regulate, to contain, to love – the process, the person, the story, and the work. Lisa Mortimore, PhD, RCC
The Polyvagal Theory (PVT), developed by Dr. Stephen Porges, is a neurbiological theory that brings significant shift in our understanding of the treatment of trauma, helping therapists understand how the Autonomic Nervous System (ANS) influences our responses to trauma, stress, social interactions, and affective and physiological regulation. Most significantly, it introduced therapists (and the world) to the concept that trauma forces the ANS into a neural state of immobility by involuntarily inciting the Dorsal Vagal System (DV), the unmyelinated, ancient part of the vagus nerve that is associated with immobilisation. Prior to Porges’ PVT, trauma was (and in some cases still is) misunderstood simply as an engagement of the fight flight response of the Sympathetic Nervous System (SNS).
In speaking or thinking about trauma, we understand that the neurophysiological self responds to traumatic experience by involuntarily shifting the ANS state. This shift is incited through the perception of threat that overwhelms the ANS and psyche, therefore it is not necessarily caused by the event, but is the result of our inability to stay safe, or feel safe, during the experience. There is an overwhelm to the system and its integrative capacities which disrupts the ability for the individual to metabolise the experience at the time.
We used to understand the ANS as two systems, the sympathetic and parasympathetic, but the PVT indicates that there are multiple states (poly) within the parasympathetic. To understand trauma we want to think about two of those states, the ventral and dorsal vagal states, both part of the parasympathetic system.
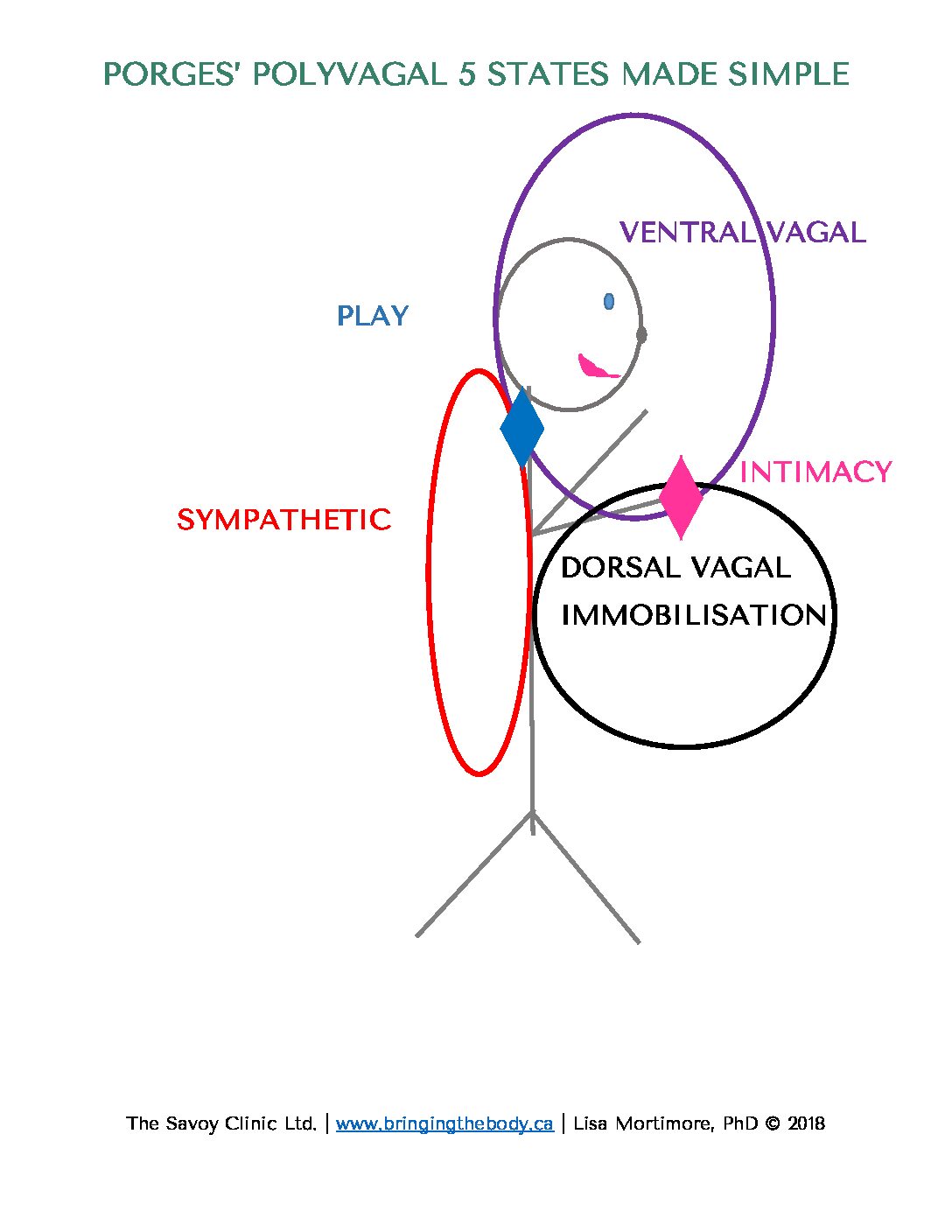
The PV theory proposes that our bodies use a hierarchical system of responses, with the ventral vagal system being the most evolved and socially engaged, followed by the sympathetic system for more intense stress situations, and finally the dorsal vagal system as a last resort in extreme danger. It also includes two hybrid systems which combine states of the ANS as in play and intimacy (see image below). The Polyvagal Theory asserts that the psyche operates out of different ANS states – in the moment of experience, as well as an overall generalised pattern or tendency, and our autonomic state is “a neural platform for behavior and psychological experiences, including feelings of being safe” (Porges, 2017, p.41). We also know that our autonomic state correlates with probabilistic behaviour and psychological feelings (Porges, 2017). We use unconscious neural processes to evaluate risk/safety in our environment.
Social Engagement (Ventral Vagal) System: This branch is associated with feelings of safety and connection. When it’s active, we are more likely to engage with others, communicate effectively, and experience positive emotions. It supports social interaction and emotional regulation. We use engagement of this system to downregulate or upregulate the ANS in trauma therapy.
Fight or Flight (Sympathetic Nervous System): In this state of high sympathetic arousal we move into fight and/or flight behaviour. Our heart rate increases and our body mobilises in ways to defend & protect ourselves.
Immobility (Dorsal Vagal) System: This branch is associated with immobilisation – ranging from the feigning of death to the inability to mobilise a response/defend or escape and dissociation. When this system is dominant, it can lead to feelings of helplessness, dissociation, and emotional shutdown. It’s a survival response to extreme threat or trauma.
Play (Ventral Vagal and Sympathetic) : This is a hybrid state, engaging both sympathetic arousal and ventral vagal, however defensive mobilisation is down-regulated through face-to-face connection or vocalisations that maintain the connection and neuroception of safety – indicating that play has not shifted into aggression.
Intimacy (Ventral Vagal and Dorsal Vagal) : This is a prosocial state, a state of social/self engagement but requires a reduction in movement. When we involve the social engagement system, “we can even use the oldest system, which is immobilization, and we can be in the arms of someone we feel safe with” (Porges, 2017, p. 129).
We have to remember that these systems regulate the ANS in adaptive responses from the most recent to the most ancient – social engagement (the ventral vagal – VV), mobilisation (SNS), immobilisation with fear (DV). The PVT tells us that under threat or when unsafe, the ANS involuntarily shifts into a dorsal vagal dominant state which decreases arousal in terms of mobilisation and reflects a survival response (Porges, 2004).When the DV system is dominant, we can see a range of effects from a collapsed sense of self to tonic immobility depending on the event; the history, and the experience(s) of the person, and can lead to feelings of helplessness, hopelessness, shame, and dissociation. Porges refers to this as a portal to the death state (2017), however, when people survive the trauma (as most do), their DV often remains active in the ANS. Porges tells us that once the survival system (DV) is engaged, it “doesn’t have an efficient pathway to get out of it” (Porges, 2017, p. 106) thereby wreaking havoc in the ANS, and can create ongoing emotional, relational and physical or physiological symptoms.
Hopefully, this brief overview of the PVT has offered some insight into the workings of the ANS, particularly as it relates to trauma. Of course, understanding it and integrating it into your clinical practice are two different things. If this has piqued your interest, know that we work intimately with the PVT in our Bringing the Body into Practice trainings and workshops.
We met with our web guru David Michels fromGeeks on the Beach and he invited us to give our readers a peek behind the scenes. We thought, hmmm, this might be fun, and even more fun, we decided to write each other’s bios and include a glimpse from behind the scenes. So, here it goes, meet Lisa Mortimore, PhD and Stacy Adam Jensen, MEd and Riley …
Lisa Mortimore is the driving force behind the Bringing the Body into Practice, Somatic Attachment Psychotherapy training- a training that is the ever-evolving synthesis of her clinical will and wisdom. In addition to weaving her heart and soul throughout her teaching, she brings to the program clinical and academic rigor, a tremendous capacity to work relationally and translate that into her clinical teaching, and a strong side of laughter. I appreciate the way she’s always pushing her clinical understanding- forging new connections and bridging between diverse clinical knowledges. It is a true pleasure to witness Lisa’s capacity to bring her heart and care into her clinical teaching, and see the fruit come to bear as students embody and deepen their practice across the two-year training. On the one hand she holds the vision what is possible, and in the other hand she lets it unfold, inviting therapists to make the material their own.
When Lisa isn’t teaching, writing, or formulating new clinical connections, you’ll find her with her hands in the mud on her pottery wheel, riding her bike, or practicing culinary alchemy in the kitchen (that’s a fancy way of saying- cooking without a recipe).
The first thing I want to say about Stacy is that he’s all heart, clinically and personally. What I mean by that is that he leads, understands, and relates through his heart. I think this is what sets him apart from other therapists and educators that teach about insecure attachment and chronic shame. Stacy works hard to bridge learners into not only relating to those who have chronic shame, but as he says, “the goal in my teaching is to humanize those who suffer with chronic shame”. Over and over again, I’ve seen how this stance, his orientation, opens therapists’ hearts as they engage with the material and that open heart extends into their practices. It’s like he pedals kindness and preaches belonging, definitely salve to those who suffer from such difficult experiences of non-recognition, misattunement, and shame.
As an educator and therapist, I see the way Stacy formulates and responds to human suffering in ways that relay, I get it and I get you, but there’s a way that he goes beyond that, to relay, and together we can find our way to solid ground. I appreciate that ground because he also brings it to our work, so when things get a little chaotic behind the scenes, when the cat needs feeding, someone’s at the door, and we are teaching online, oh, and what are we going to eat for lunch, he brings it down a level, and Riley (the cat) gets fed, and so do we 😊
When Stacy’s not mucking about with clinical material, teaching, or in his practice, he’s living life on two wheels, bicycle wheels that is.
You’ll also note the black feline in the illustration, that’s Riley, she’s pure sweetness, and occasionally makes an appearance at the trainings (online), to make sure us humans have things under control.
So that’s us, a little peek behind the scenes of the BBP trainings.
As a lifelong cyclist I know the harrowing things that can happen when we live life on two wheels. The good thing is that as a psychotherapist specializing in trauma, I know some of what it takes to process the trauma of accidents and near misses. I’m going to outline the simplest thing that we can do so that the fright of a near miss doesn’t get stuck inside our body, and compromise our ability to be safe on the bike.
Here’s a common scenario- you are riding and someone opens their car door right in front of you. Your natural reflexes take over and you slam on your brakes, swerve into the next lane, or so some variation of the two. Thank goodness, you don’t hit the door and there was no car in the next lane, so you were lucky and had only a close call, not a physical collision and trauma. As you stop, your heart is racing, and you may be enraged, or afraid, or even terrified; your heart pounding and pulse racing, and your body feeling both shaky and energized. Your sympathetic nervous system has mobilized to get keep you safe (fight/flight), and it has been fused with the shock from the opening of the car door. The evasive action that you took in that split second to avoid injury or possible death, though successful, isn’t enough to discharge (release) the tremendous amount of energy created by the situation, which gets bound up in the body and nervous system.
If you do as many of us probably have done, many times- you say ‘phew’ (or some variation), or educate the driver about how to open a car door properly, or pause for a few moments, then continue on with your ride. As you ride, you may feel shaky, nervous, easily startled, like your balance is a bit off, or maybe a bit ‘out of it’- like you can’t take in all the information in your surroundings, be it cars (moving or parked), potholes, etc., and things can startle you. If you have a close call while riding gravel, cross or mountain biking, you may find that you keep crashing, or almost crashing. All of these things add up to having a bad ride, and being at increased risk of injury.
The culprit for this strong reaction and resulting vulnerability is your nervous system- which did what it was meant to do- to keep you safe, but hasn’t had the time to come back to equilibrium. After the shock of the incident our nervous system needs time to settle, to metabolize, to discharge all of the shock and survival energy that was just created, and we don’t often allow this to happen, interrupting the body’s natural rhythm. In the above example, we halted the discharge/settling process by simply continuing the ride, or it could be by checking Strava, or sending a text, etc. All of which keep us distracted, and unaware of what is happening in our body- unaware of or disavowing the intense activation present in our nervous system.
Here’s how to do it differently. The next time you have a near miss or something else that frightens you- get to safety (so off the road or trail), and take a moment to notice things that help you orient to the here and now (I see a tree, I feel the cool breeze, I smell cut grass, I hear a crow calling, my friend is sitting with me, etc.). Now, take some time to give your body and nervous system space- be curious about what is happening inside, and give it space to express itself. This process may feel very odd and vulnerable, and as you do this, you may experience a rush of heat or cold, or you may feel some shaking, your face may flush, or you may feel some fear- some tears may come, or even some nervous laughter. All of these are signs that the shock to your system from the near miss is processing and your body is moving it through. The point is to give your body space to express itself- to do what it naturally wants to do- to allow the bound-up survival energy to come out, so that you don’t have to carry it with you for the rest of the ride, and possibly beyond. The good thing is that this process described above only needs a few minutes to happen, and once this wave has come through, your system will naturally settle- you will feel more grounded, present, focused, and ready to go on with your ride. The discharge of the energy may not be entirely complete, so when you get home, give your system some space to see if anything residual is left, by repeating the process I’ve laid out above.
I’m aware that the process I’ve laid out above doesn’t fit well with the culture of many group rides, and it would be great if this could shift. Educate your riding friends, and if you are on a group ride and are unable to give your nervous system time to discharge in the moment- do it as soon as you can afterwards, once you get home, or at the post ride coffee- before the energy has become really rooted inside your system.
If you do get hit or injured, or have a bad crash on your bike (or anywhere) and are dogged by the incident, reach out to a trained therapist that can help you move the residue from the accident – check out our referral list – https://bringingthebody.ca/referrals/.
I hope that this information is helpful, and that you take up the challenge to listen to your nervous system after your next close call- your nervous system will thank you for it. Have a safe ride.